Retake
C21) Worsening dyspnea and cough in a metal foundry worker
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a pediatric patient with shortness of breath.
- Review the DDx considerations in a pediatric patient with shortness of breath.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating a pediatric patient with shortness of breath.
History
A 59-year-old male visits his primary care provider for a routine checkup. He reports worsening dyspnea and non-productive cough over the last few months, with breathing difficulties during prolonged walking or exercising on his stationary bike. He has worked at a metal foundry for the past 7 years and only occasionally wears a mask. He denies chest pain, palpitations, wheezing, hemoptysis, or recent travel.
Physical Exam
BP: 136/82, HR 82, RR 22, Temp 98.6°F, O2 saturation 91% on room air
HEENT: No cervical adenopathy.
Cardiovascular: Regular rate and rhythm, no murmurs, rubs, or gallops. Normal S1, S2 across the precordium. 2+ dorsalis pedis and radial pulses bilaterally. No carotid bruit. JVP 2 cm H2O above the sternal angle.
Pulmonary: Fine crackles at bilateral lung apices. No wheezing or rhonchi. Coughing during the exam.
Extremities: No pedal or pretibial edema.
Labs
Spirometry:
• FEV1: 3.00 L (66% predicted) - Below normal
• FVC: 3.50 L (70% predicted) - Below normal
• FEV1/FVC: 0.90 - Elevated
• TLC: 4.50 L (72% predicted) - Below normal
• DLCO: 60% predicted - Below normal.
CBC: Within normal limits.
D-Dimer: Within normal limits.
Provisional Diagnosis
Select the Dx you believe is most appropriate
Pneumoconiosis is the most appropriate diagnosis given the patient's gradually worsening dyspnea and cough, age, and history of occupational exposure to inorganic, fibrogenic particles. Spirometry values (reduced FEV1, FVC, and TLC with elevated FEV1/FVC) suggest a restrictive, rather than obstructive, lung disease pattern.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
Given the likely diagnosis of pneumoconiosis, acuity is routine.
First Imaging Study
What is the first imaging study you will order?
A chest X-ray is an appropriate first imaging modality in this case, as it is relatively inexpensive and can be obtained quickly.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
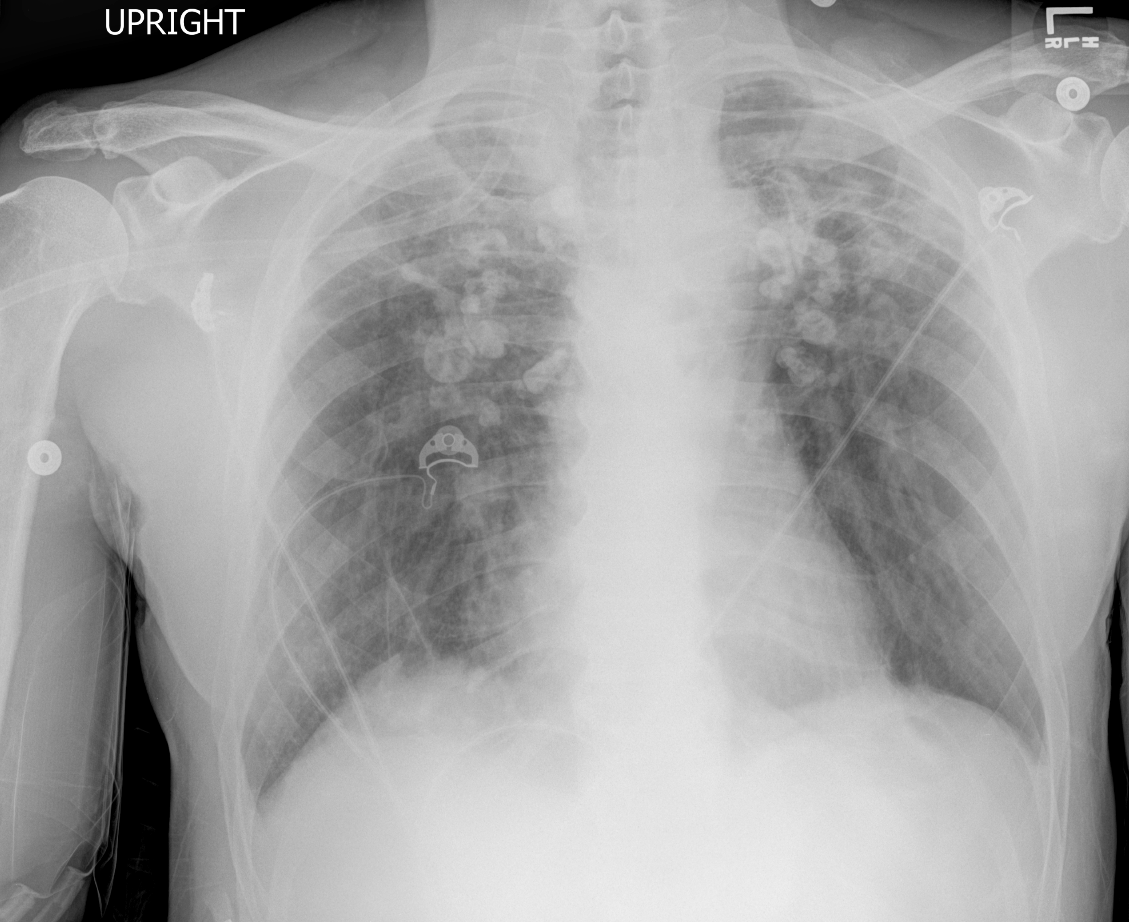
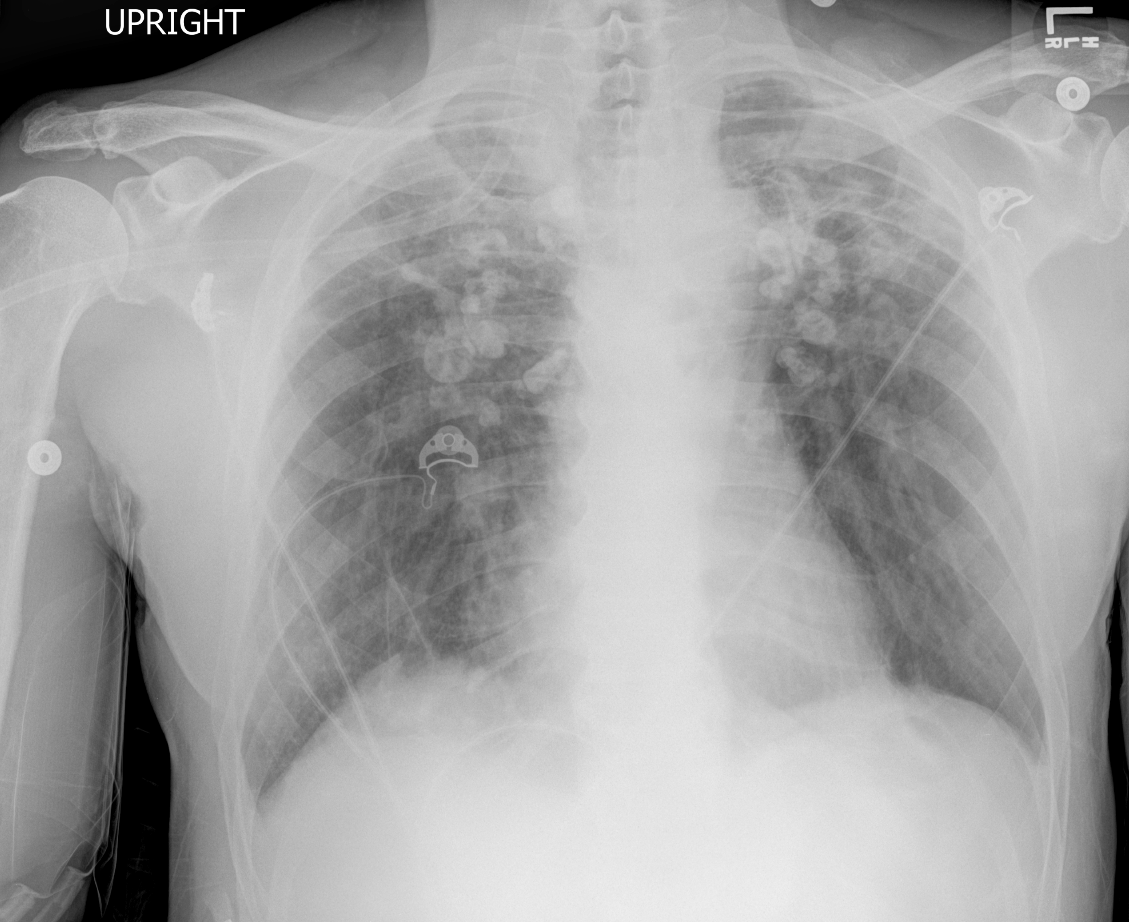
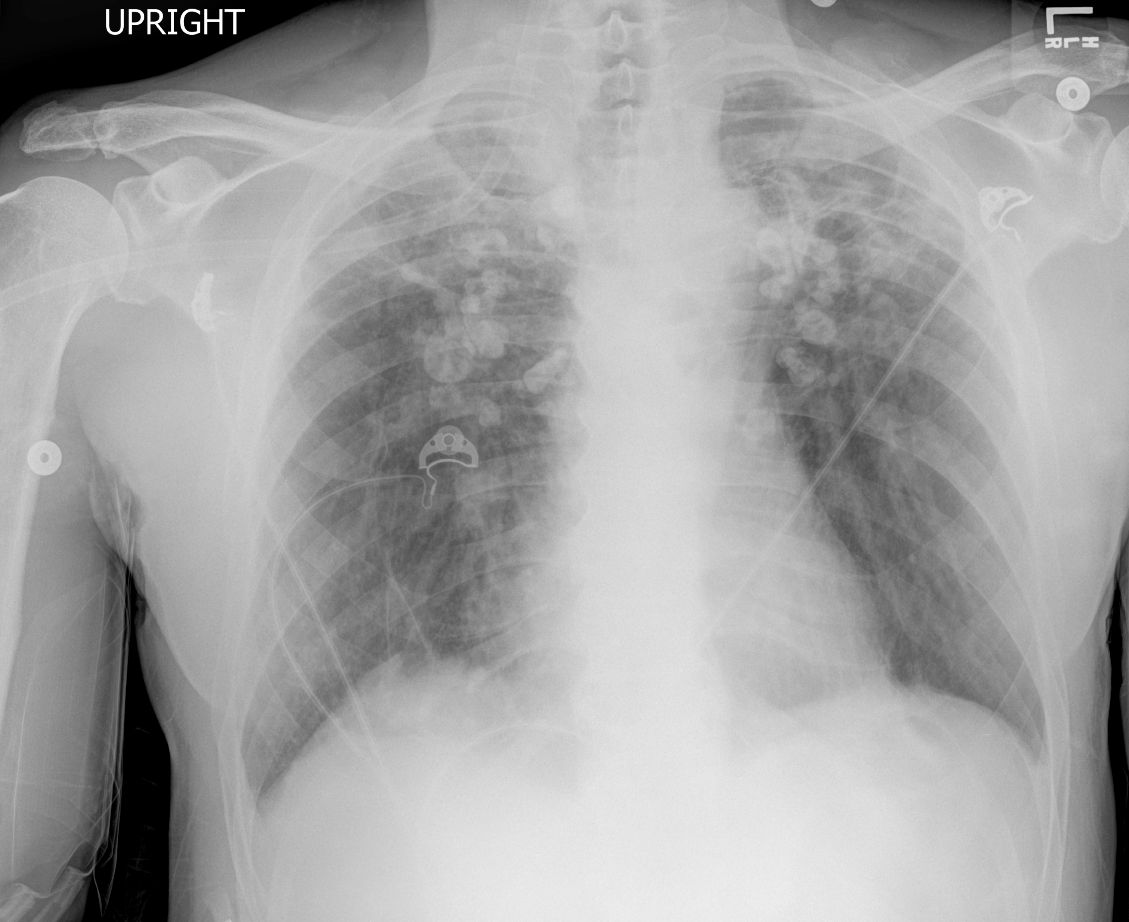
Chest X-ray
There is fibrosis at the:
Fibrosis is present at the lung apices bilaterally.
There is cardiomegaly.
The cardiac silhouette appears normal in size. It does not occupy >50% of the chest wall diameter.
Describe the hila of the lungs.
Bilateral hilar lymphadenopathy with peripheral "eggshell" calcification is present.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
A high-resolution CT scan can further characterize disease of the lung parenchyma and differentiate silicosis from other pneumoconioses.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
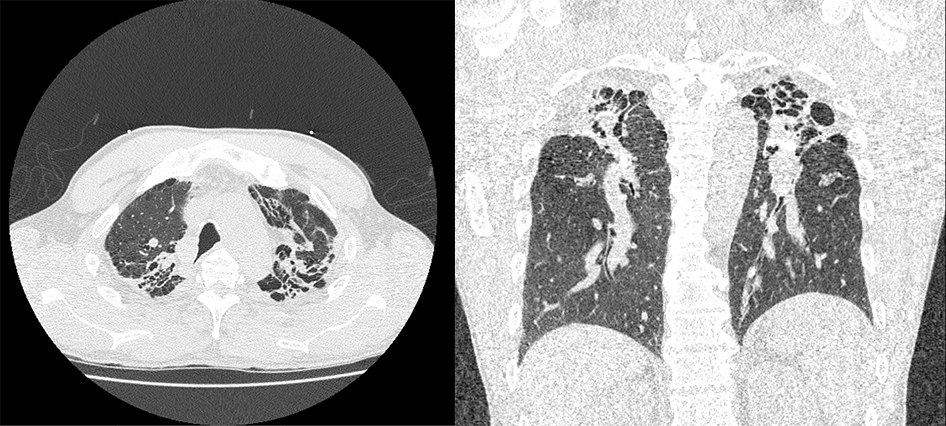
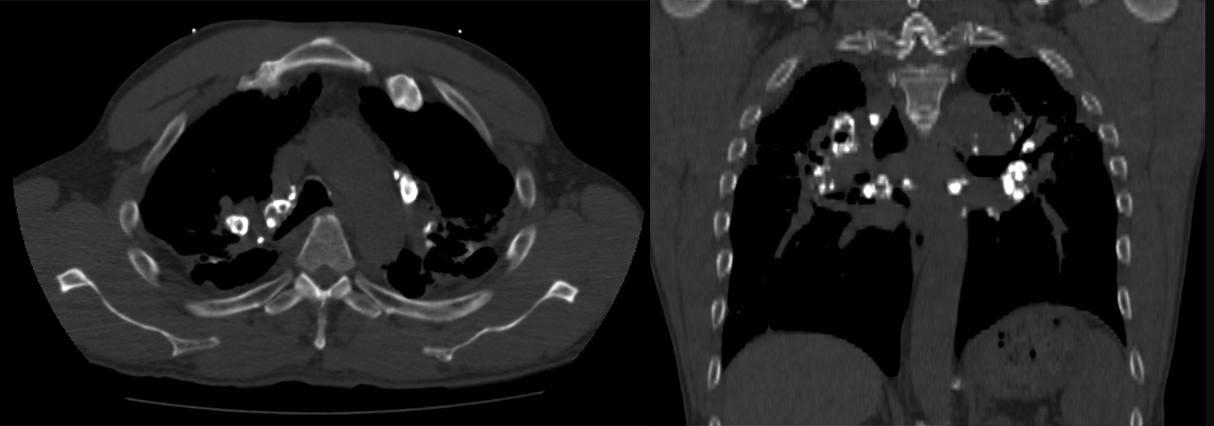
HRCT
Peripheral calcification of the hilar lymph nodes is present bilaterally.
There is peripheral calcification of the hilar lymph nodes bilaterally.
View the full study if you'd like to like a look yourself
Third Imaging Study
What is the next imaging study you will order?
No further imaging is needed, as the diagnosis is strongly suspected with the imaging findings.
What is your Diagnosis now that you have seen the imaging results?
Silicosis is the most likely cause of this patient's shortness of breath and cough, given his history of working at a metal foundry, restrictive pattern on spirometry, peripheral lymph node calcification, and fibrosis of the bilateral upper lung fields.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
This patient's condition is not life-threatening and can be managed routinely.
Assessment and Plan
Please provide your assessment and plan for this patient
A 59-year-old male with a 7-year history of metal foundry work presents with several weeks of dyspnea, dry cough, and bilateral crackles on exam. Spirometry shows a decline in lung function and preserved FEV1/FVC ratio. Chest X-ray and HRCT findings of eggshell lymph node calcification and upper lobe fibrosis confirm the diagnosis of silicosis, a restrictive interstitial lung disease without a cure.
Management will focus on preventing exacerbations and slowing the progression of lung fibrosis. The patient will be referred to a pulmonologist. Management may include supplemental oxygen as needed, smoking cessation counseling, immunization against influenza virus and pneumococcal pneumonia, and use of antifibrotic agents. The patient may also require regular monitoring of lung function and pulmonary rehabilitation. It is essential to educate the patient on avoiding further exposure to silica dust and emphasize the need for ongoing surveillance for potential complications, including tuberculosis and lung cancer.
Lessons Learned:
- Pneumoconioses are a group of restrictive lung diseases caused by occupational exposure to inorganic, fibrogenic particles.
- Silicosis, a type of pneumoconiosis, results from exposure to crystalline silica, which is common in professions such as sandblasting, metal foundry work, glass production, mining, and construction.
- In restrictive lung disease, the FEV1/FVC ratio is often normal or elevated.
- Chest radiography is the most appropriate initial imaging modality for suspected silicosis, with common findings including bilateral hilar lymph node "eggshell" calcification and biapical fibrosis.
- HRCT may provide additional information on the extent of lung involvement and complications.
- There is no definitive treatment for silicosis; management focuses on improving symptoms, preventing exacerbations, and slowing progression.
- Patients diagnosed with silicosis are at a higher risk of tuberculosis infection due to the disruptive effects of silica on macrophage phagolysosome function.
Socioeconomic Factors: Silicosis is an occupational hazard that predominantly affect workers exposed to crystalline silica in technical and production jobs. Providing proper education about these conditions, implementing safety precautions to limit inhalation of these particle, and ensuring access to appropriate protective equipment is crucial for protecting workers' health.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Next


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}